

Excess Mortality Post-Vax – a Cross-country Study
Excess mortality has been elevated after the roll out of the vaccines. Can we make anything of that?

A few weeks ago, I posted a result about how peaks in excess mortality in the United States appear to lag peaks in self-reports to the Vaccine Adverse Effects Reporting System (VAERS). Spooky. Did people perceive “adverse effects” and then, five months later, did some share of those same people experience the ultimate adverse effect?

That might make for an ambitious conclusion, but, yes, it’s spooky. That said there are two things we can say. First, country-by-country, excess mortality edged up significantly after the roll out of the vaccines. Is there a connection? Second, the rate of vaccinations in each country tend to exhibit at least two conspicuous peaks. (These peaks may reflect a first wave of vaccinations followed some months later by a round of second vaccinations or boosters.) There is some suggestion in the data that peaks in excess mortality lag the peaks in vaccination by about six months. Is there a connection?
I am going to suggest that it is hard to establish connections to anything with publicly-available data. It would help to get access to individual-level data to identify vaccine effects, positive or negative, lagged or immediate, in the mortality statistics. That said, post-vax excess mortality is elevated. Indeed, post-vax, non-COVID excess mortality is elevated. Something is going on. Various things may be going on, but are the vaccines inducing lagged effects, and could we identify such effects? We read almost any day of someone young and healthy “suddenly” suffering “cardiac arrest.” Even so, we cannot obviously expect the health authorities to sort things out for us—not without being compelled.
I downloaded the COVID database from Our World in Data, and I ran a regression that mapped excess mortality against lagged values of the volume of vaccinations by country. I consolidated the data by month, because countries that report excess mortality tend to report it by month.
Not all countries regularly report excess mortality or vaccination numbers. Accordingly, almost all of the African countries disappear from the analysis. These same countries tend to support much younger populations, and younger populations are just the populations least likely to perceive much effect from COVID. But, what of the older, more developed countries?
One version of the analysis accommodates country-specific attributes by coarsely controlling for them by assigning a dummy variable to each country. (This was a “fixed effects” analysis.) A parallel analysis puts a little more structure on country-specific effects by replacing dummy variables with GDP per capita and Median Age in the regression. The two analyses bracket the following results:
On average, countries experienced an increase in monthly excess monthly between 6.4% and 8.4% after each country rolled out the vaccines. That is a sizable increase, notwithstanding the fact that it is much more conservative than some of the numbers other observers report.
Excess mortality may exhibit cycles. So do vaccinations, although vaccinations run counter to the cycles in excess mortality. Specifically, the 2nd or 3rd-month lag in vaccinations may, on average, show up as negative and significant. The 6-month lag shows up as positive. That is, peaks in excess mortality tend to match up with the peaks in vaccinations that are lagged by six months.
What to make of all of that? Some observers have articulated complex mechanisms like “antibody dependent enhancement” or “original antigenic sin” that could explain how vaccinations enhance the prospect of COVID infections (if not mortality). At the same time, observers worry about (potentially fatal) adverse effects like myocarditis, especially in otherwise healthy young people.
Do the regression results prove anything? Not really. We already knew that the vaccine campaigns have stopped neither COVID infections nor COVID fatalities. But, do the vaccines induce fatalities whether by COVID or by other channels? It is hard to disentangle what is going on.
That said, I will show the reader some (non-randomly selected) graphical results. Let’s first look at Australia:
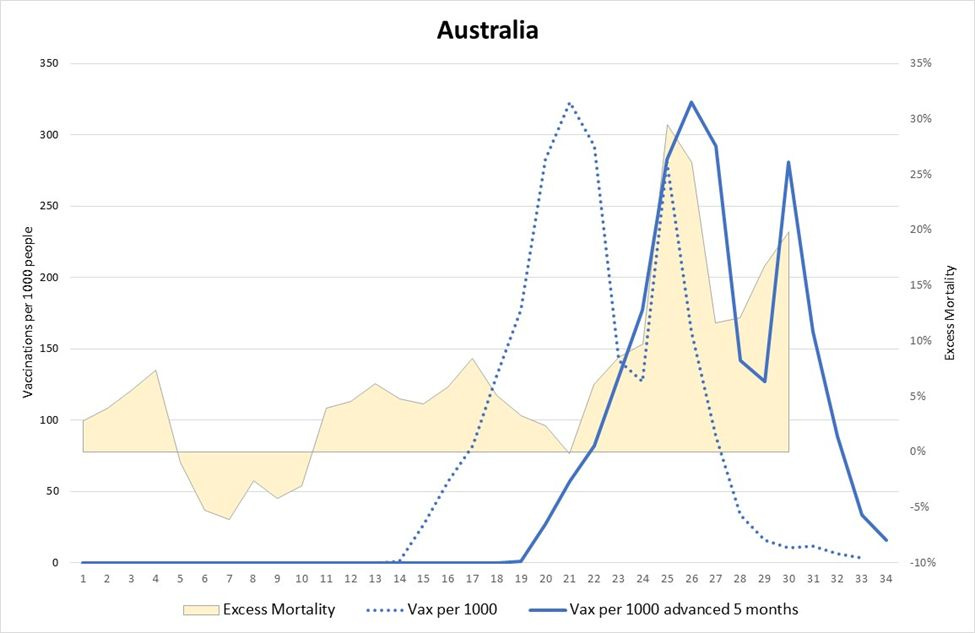
The dashed blue line indicates the vaccinations per 1,000 people (by month). The solid blue line indicates vaccinations shifted five months into the future. The yellow area indicates excess mortality (%). These data are mapped across as many as 34 months starting in January 2020 and running into late October 2022.
The question is: Do the solid blue line and the yellow area roughly line up?
The Australia result is certainly suggestive. At the very least, it is hard not to observe that excess mortality became elevated some months after the public started to get access to the vaccines. What was going on?
Let’s look at the United Kingdom:
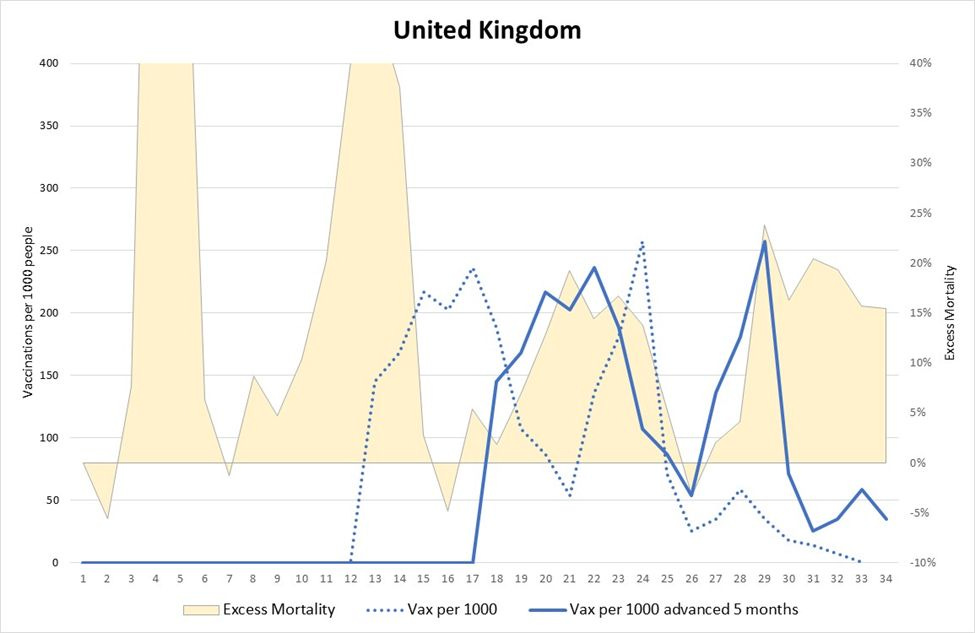
Mortality had exhibited episodes of elevated excess before the vaccine rollout, but the five-month lag in vaccinations roughly lines up with successive peaks in excess mortality. Interesting.
Brazil?:
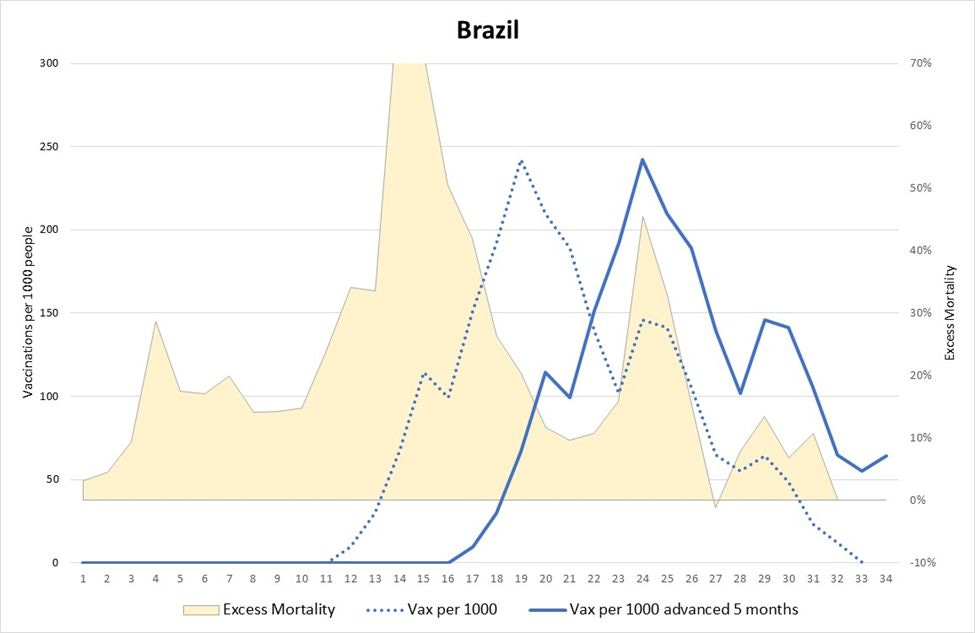
Excess mortality had already been elevated, but, again, vaccination (lagged five months) roughly line up with patterns in excess mortality post-vax.
Japan is a little different:

Excess mortality had been running mostly negative pre-vax (average -3.5%) but started running positive post-vax (average 2.7%). Did the vaccines have something to do with that, or was it just the case that COVID had finally caught up with Japan just as it had in Australia? Or, had excess mortality been trending upward all along for reasons that have had little to do with the vax?
These data are not sufficient to sort out such questions, but there is a five-month meme floating around. The results presented here derive from the experience of 101 countries, and these data suggest that there may be a six-month lag in the data. So, at the very least, one can imagine that some observers would speculate about connections between the volume of vaccinations and mortality statistics. But, again, I would argue that such conclusions are not litigation-ready. We await analyses that work out of individual-level data.
If something quite specific at 5 months were happening then it seems the type of the vaccine would matter. UK was primarily Astra Zeneca in the early stages, others I suspect not. Given the different underlying principles of the vaccine it would seem odd to see the same exact pattern. Can we compare only countries using the same vaccines?
Others have observed the same effects. Ought ti raise alarms within the NIH. Are they all bought?