

The COVID Children’s Crusade
Slaughterhouse 2022

In his semi-autobiographical account, Slaughterhouse Five (1969), Kurt Vonnegut recounts being captured by the Germans during the Battle of the Bulge (1944) and then enjoying the privilege of joining POW's assigned to work in Slaughterhouse 5 in Dresden. The POW's ended up enjoying the greater privilege of being on the receiving end of the infamous firebombing of Dresden in 1945.
Kurt Vonnegut and his friend Bernard O'Hare made it out intact and eventually made it home by way of a Soviet prison camp.
Years later Vonnegut looked up his “old war buddy” O'Hare. He wanted to take some time with O'Hare to recount some of their experiences in the war. Those experiences would inform a book he had been struggling with.
“You were just babies in the war,” exclaimed O'Hare's wife Mary. This notion of “babies” going off to war got the three of them -- Kurt, Bernie and Mary -- thinking about the "The Children's Crusade":
O’Hare looked it up in a book he had, Extraordinary Popular Delusions and the Madness of Crowds by Charles MacKay [1841]… [T]he Children's Crusade started in 1213, when two monks got the idea of raising armies of children in Germany and France and selling them in North Africa as slaves. Thirty thousand children volunteered, thinking they were going to Palestine...
Through a misunderstanding, some children reported for duty in Genoa, where no slave ships were waiting. They were fed and sheltered and questioned kindly by good people there -- then given a little money and a lot of advice and sent back home.
“Hooray for the good people of Genoa,” said Mary O'Hare.
The complete title of Slaughterhouse Five is Slaughterhouse-Five, or the Children's Crusade: A Duty-dance with Death.
Are not the public health authorities world-wide and their enablers in the political class intent on engaging a new Children’s Crusade? Specifically, does it really make sense to push the “vax” – the mRNA therapies – on young people?
In this short note I pose a very conservative estimate of the fatality rate for young people. I use data from the Centers for Disease Control (CDC). These include data from VAERS, the Vaccine Adverse Effects Reporting System (maintained and vetted by the CDC as well as by other entities), to pose a conservative estimate of the risk of dying from the vax.
The result?
For every young person we save, we kill at least another eight and maim yet another nine.
If we vax 30 million young people in the United States, we end up killing at least 1,200 of them in order to save 150. Moreover, we end up maiming another 1,300 to save that 150. It gets worse. That 150 would tend to be very unhealthy people whereas that 1,200 who would die or the 1,300 who would be maimed tend to be healthy young adults. We’re killing and maiming a sizable number of healthy young people in order to save a much smaller number of unhealthy young people.
How do we generate such results? It would be helpful were the CDC to furnish uncensored access to data on vaccinations and “confirmed” COVID cases. And, ideally, we would be able to identify unconfirmed cases of COVID infection. How many people were infected and never knew it? Or maybe they perceived some symptoms but stayed home and took care of themselves rather than venture to the hospital or get tested?
As it is, the CDC only affords access to highly censored data. In this note I refer to three data sources:
(1) The January 5, 2022 edition of “COVID-19 Case Surveillance Public Use Data with Geography” maintained by the CDC Case Surveillance Task Force. The entire dataset of 42 million records can be downloaded at https://data.cdc.gov/Case-Surveillance/COVID-19-Case-Surveillance-Public-Use-Data-with-Ge/n8mc-b4w4.
(2) The January 10, 2022 edition of “COVID-19 Vaccinations in the United States, Jurisdiction” maintained by the CDC at https://data.cdc.gov/Vaccinations/COVID-19-Vaccinations-in-the-United-States-Jurisdi/unsk-b7fc.
(3) The December 31, 2021 edition of the entire VAERS dataset at https://vaers.hhs.gov/data/datasets.html.
The main thing to get from the VAERS data is that they indicate 11,421 fatalities over a body of 746,944 reports of adverse effects in the United States and territories relating to COVID vaccines. Of these reports, over 54,000 involved hospitalizations, and another 12,819 indicated severe disablement.
Now let’s turn to vaccination numbers. It would be good to know the age distribution of all doses of the mRNA vaccines, but the best we can do with available data is generate some raw counts of doses. The vaccination data indicate the administration of more than a half-billion doses in the United States & territories as of January 8, 2022. That makes for 1.56 doses per person. Most people have been vaxxed, and most of those people have secured more than one dose.
We can now calculate a very conservative fatality rate from vaccination. Suppose that, on average, a person who has taken the vax has absorbed two doses. Some will have only secured one dose. Others will have secured the “booster” (a third dose). But, if the average is two doses, and 518 million doses have been administered, then about 260 million people will have secured a dose at some point. That is our denominator: 260 million. We already have our numerator: 11,421 fatalities. The ratio of fatalities to number of vaxxed people is 0.004391%, a small number. That is, if we take this number as a “Vax Fatality Rate” (VFR), we get a VFR of 1-in-22,772. The likelihood of dying from the vax is a little lower than the likelihood of being murdered in the United States (as of 2019 per data from the FBI).
Some observers will argue that VAERS notoriously under-represents adverse effects, including fatalities. It’s hard not to believe that that is true, but the point here is to pose a very conservative estimate – a conservative lower bound – on the likelihood of dying from the vax. A rate of 1-in-23,000 is conservative.
Observers will also note that this lower bound of 1-in-23,000 does not control for age. It could very well be the case that very young people are more susceptible to adverse effects. That may very be true, but absent any means of controlling for age, we pose the unadjusted rate of 1-in-23,000.
We now turn to the CDC’s COVID surveillance data for a conservative estimate of the fatality rate from COVID for young people aged 0 – 17. Of 42 million reports, about 27 million are censored. The remaining 15-million-plus reports yield the following cross-tabulation of death attributed to COVID against age cohorts:
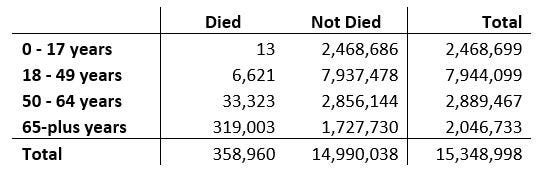
Fewer than 1-in-189,900 young people aged 0 – 17 who contracted COVID ultimately succumbed to COVID. That is, a conservative estimate of the likelihood of succumbing to a COVID infection for a young person was less than 0.00053%.
We can now do a risk-benefit analysis. Suppose the vax saves one in 189,900 young people but kills one in 22,772 and maims one in 20,288. Thus, our result:
For every young person aged 0-17 the vax saves, the vax kills more than 8 others and maims more than another 9.
That is a heavy toll, more than seventeen young lives shattered to save one (likely very unhealthy) young person.
Let me pose the hazards of vaccinating young people as but one dimension of a COVID Childrens’ Crusade. Another would be the larger toll of the public policy response to the COVID phenomenon. Since the beginning of the pandemic in early 2020, young people under the age of 24 have been dying at a rate far in excess of the rate experienced in the previous several years. Data from the CDC demonstrate that we cannot attribute most of this “excess mortality” to COVID.
“Excess mortality” is a very useful measure of performance. It itself does not require us to assign causes of death. We need only count up fatalities. Numbers of fatalities are hard to misrepresent whereas attributing causes of mortality can make for a tricky business.
Calculating excess mortality involves coming up with a benchmark of expected mortality in a given year. There is no unique way to do this, but here I adopt a method deployed by the CDC: we take the average of weekly mortality for the years 2015 – 2019 and compare that to actual mortality in 2020 and 2021. See the following graph:
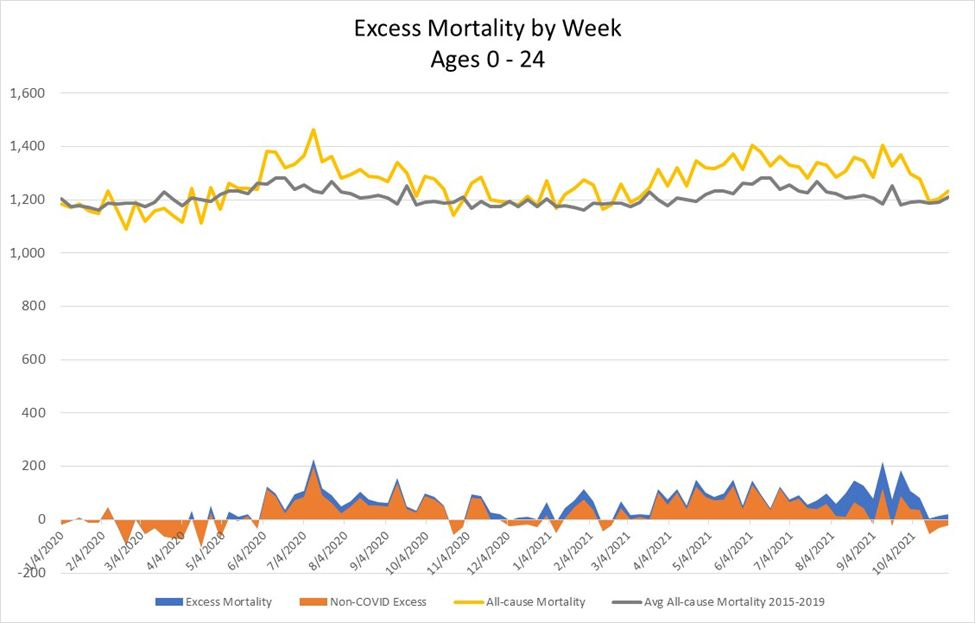
The yellow line indicates actual mortality in 2020 and 2021 (by week through October 30, 2021) and averages above 1,200 fatalities per week for young people aged 0 – 24. The grey line represents benchmark mortality. The difference between benchmark mortality and actual mortality is “excess mortality” (the blue area at the bottom of the graph).
The orange area indicates excess mortality absent fatalities attributed to COVID. The striking feature of it is that Non-COVID excess mortality starts running mostly positive starting in June 2020. Indeed, in the two-year interval 2020-2021, excess mortality not attributed to COVID has averaged more than 28 fatalities per week for young people aged 0 - 24. Meanwhile, total excess mortality averaged 53 fatalities per week. In other words, causes other than COVID alone account for more than half of excess mortality for young people. Indeed, that non-COVID excess alone indicates mortality more than 20% above the rate of mortality that would have been expected. Something is going on that cannot be attributed directly to COVID. Instead, young people have been dying at a 20% higher rate, absent COVID, because why? I leave it to the reader to speculate, but public policy, including the closing of schools and universities would make for a good place to start. The denial of early-career jobs would be another good place to look.
The data for this last exercise derive from the January 6, 2022 edition of “Provisional COVID-19 Deaths by Week, Sex, and Age” provided by the National Center for Health Statistics and posted at https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-by-Week-Sex-and-Age/vsak-wrfu.
The world has now more than two years’ experience with the coronavirus phenomenon, but public health authorities cannot demonstrate the efficacy of any measures to contain or slow the diffusion of the virus. Indeed, as of the writing of this short note, some authorities are beginning to recognize that COVID is now endemic. (The observations of Ezekiel Emanuel and coauthors in the Journal of the American Medical Association are apposite.[1]) We have to live with it, they observe. The fiction of “Zero COVID” is just that: a fiction. What we can discern, however, from our censored, unprivileged perspectives on public health data, are sharp indications that young people have been made to suffer grievously through these two years. Better access to data would afford some means of better characterizing how they have suffered, but for now we are stuck with what many of us have surmised all along: public policy has failed to protect the public and has actively harmed many.
So, where are the good people Genoa to give young people a kindly talking-to and the public authorities the obvious criticisms that they deserve? That criticism would include the fact that the decision to fetishize COVID fatalities was just that: a decision. We don’t fetishize fatalities attributed to flu viruses that annually kill more young children than COVID. Nor have we fetishized other viruses, including other coronaviruses, that cause the “common cold”. SARS-CoV-2 (“COVID”) will now join those other viruses in seasonal circulation. That said, Emanuel and coauthors seem to be setting us up to start fetishizing all viruses. The authors recognize that “Zero COVID” is infeasible but then call on the authorities to devote more resources to the surveillance of virtually all viruses. But, to what purpose? Do Emanuel and coauthors contemplate permanent “vaccine passports” or even a larger “social credit” surveillance system? Can the good people of Genoa anticipate and suppress efforts to expand an already failed public health policy regime?
[1] Emanuel, Ezekiel, Michael Osterholm, and Celine Gounder, “A National Strategy for the ‘New Normal’ of Life with COVID,” Journal of the American Medical Association, January 6, 2002 at https://jamanetwork.com/journals/jama/fullarticle/2787944.
An extremely well-written piece. After looking at the data, anyone who continues to push mRNA "vaccines" on young people is, in my opinion, nearly guilty of involuntary manslaughter.