
Is the death toll of the vaccines becoming impossible to ignore?
The COVID Children’s Crusade, Part II

What is going on?
Summary of Results —
Data from the Centers for Disease Control (CDC) show that, starting in early May, 2021, people have been dying at exponentially increasing rates from conditions involving “Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified”. The seasonal, baseline rate in a given January for such “abnormal” conditions would be nearly 700 fatalities per week, but by January 1, 2022 the actual rate had exceeded 3,000 per week and was still sharply increasing.
An obvious hypothesis is that the COVID vaccines (the mRNA therapies) have induced these fatalities. Specifically, in 2021, deaths in excess of baseline rates that the CDC attributes to “Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified” very nearly totaled 22,000. The data indicate at least another 21,000 fatalities in excess of baseline fatalities through the first eight weeks of 2022. That would put the death toll from the jab in excess of 43,000 as of February 26, 2022.
CDC data indicate that fatalities from unnatural causes in excess of baseline rates totaled nearly 20,000 in 2020 and exceeded 20,000 in 2021. These fatalities started to depart from the baseline in April 2020. It was at just that time that non-COVID fatalities among people under the age of 45 started to pick up. Absent evidence to the contrary, it is hard not to conclude that young people and people of prime working age were committing suicide or succumbing to drug overdoses or alcohol poisoning at rates on the order of 500 a week in excess of baseline rates.
CDC data indicate that nearly 850,000 people in the United States succumbed to coronavirus in all of 2020 and 2021.
Another 770,000 died “with COVID,” but not principally “by COVID,” over this same two years.
Of the approximately 1.6 million people who died either “with COVID” or “by COVID” in 2020-2021, about 630,000 would have died anyway.
One might have guessed that COVID had been taking away people who had already been on the verge of death. The last result shows that there is something to that. But this result also demonstrates that COVID did induce a non-trivial volume of mortality well in excess of the rate of mortality that could have been expected in 2020 or 2021. In 2020-2021, “excess mortality” from all sources totaled nearly 1 million. Nearly 1 million people died in 2020-2021 in excess of baseline rates, and some share of the 850,00 COVID fatalities contributed to that toll—but so did other causes of death.
The publicly available data do not allow us to specifically determine what number of people who had died “by COVID” would have died anyway, but neither is it the case that one can responsibly summarize the toll of coronavirus with such declarations as “COVID has killed 850,000 people!” Such declarations amount to unsophisticated bean-counting; they make no allowance for the fact that the COVID toll has been concentrated on immunocompromised people—on the very elderly and the infirm. Indeed, that is why the median age of death attributed to COVID anywhere in the world has persistently exceeded the median age of death from plain old death. Many of these people would have died anyway in 2021 and 2022 whether from influenza, pneumonia or a host of other conditions that afflict the immunocompromised.
The data show that deaths by influenza, pneumonia, chronic lower respiratory diseases and other respiratory conditions markedly diminished in 2020 and 2021. Such results would be consistent with the toll of COVID being concentrated on immunocompromised people who would have otherwise succumbed to these other conditions.
Some observers like to compare the COVID death toll to the death toll from war. This is silly. The death toll of war tends to be concentrated on young people. Not so with COVID. The median age of death from America’s wars has been a lot closer to 20 whereas the median age of death attributed to COVID is about 80. Big difference, and not acknowledging the big difference amounts to emotional manipulation.
Meanwhile, the CDC data show that excess mortality among young people has been persistently elevated from the beginning of the pandemic to the present.
Even worse: Most of that excess mortality among young people was not induced by COVID itself. Indeed, we can say that more than 60% of excess mortality of people under the age of 25 involves fatalities neither “with” nor “by COVID”. Something else, something very sinister, has been going on. It is hard not to suspect that poor public policy (lockdowns and such) is the principal driver of excess mortality among our youngest people as well as among people of prime working age. The vaccines themselves have likely been taking their toll, too.
We can say that the share of excess mortality attributable to COVID for people under the age of 25 is likely well higher than 60% for two reasons. First, the data do not allow us to tease out who had died “with COVID” as opposed to “by COVID”. The people who died “with COVID” likely would have died—and, in fact, did die—from some other cause, anyway. Second, even some number of people who died “by COVID” would have died anyway, but we can’t determine how many.
We can say a similar thing about people aged 25 to 44. At least 20% of excess fatalities among these people derive from causes other than COVID, and likely far more of these excess fatalities derive from other sources, because, again, some number of people who died either “with” or “by COVID” would have died anyway.
The data show that “vaccinations”—treatments with the mRNA therapies—have not stopped the diffusion of coronavirus. Meanwhile, there is some question if the vaccines themselves have induced some appreciable volume of deaths, especially among younger people.
I had taken that topic up in an earlier essay that looks at the very imperfect data from VAERS, the Vaccines Adverse Effects Reporting System. The CDC data do not tease out any finely-tuned results pertaining to vaccines, but there are strong suggestions that vaccines have taken their toll among younger people in the latter half of 2021. That would have been just when students were returning to in-person instruction at university.
I update results about relative performance across states in the United States. I examine “excess mortality” as a share of benchmark (baseline) mortality by state. The COVID phenomenon did induce excess mortality across all states, and some states may have the appearance of performing worse than others by virtue of experiencing a greater number of fatalities attributed to COVID. But, examining excess mortality as a proportion of benchmark mortality amounts to controlling for differences between states that are fixed over the course of the pandemic. Such an exercise amounts to a “fixed effects” analysis. And the analysis demonstrates appreciable convergence over time of states’ performances to the national average performance. Such a result is consistent with the proposition that the different approaches taken by the states to either control the diffusion of COVID or to just be resigned to its diffusion made no discernible difference in performance. To date, for example, Florida has marginally outperformed California notwithstanding the fact that the media have harshly criticized Florida for its more laissez faire approach to COVID and have praised California for its illiberal approach. Ultimately, the conceit that the authorities can control of virus amounts to just that: a conceit.
Introduction —
Imagine a pandemic that infects people and kills people, whether young or old, rich or poor, with equal probability. It’s like everyone draws a card from a deck. Everyone who gets a bad draw—draws the ace of spades or a joker, say—gets infected. Everyone else dodges infection. Then, everyone who gets infected draws another card from another deck. A bad draw from that second deck amounts to succumbing to the infection. Getting a good draw amounts to recovering from infection. Everyone draws cards from identical decks.
The age distribution of people who would get infected would look like the age distribution of people who dodge infection. The age distribution of people who die would look like the age distribution who survive infection… which would also look like the age distribution of the people who dodge infection. All age distributions across all outcomes would look like the age distribution of the entire population.
The same would go for any other distributions across any other dimensions; the distributions of people who die, get infected or dodge infection across race, wealth, sex, whatever, would look the same.
Has any pandemic in history ever looked like that? Approximately so?
Perhaps the waves of bubonic plague in the 14th and 6th centuries looked very roughly like that. In the “Justinian plague” of the 6th century, the emperor of the Eastern Roman Empire, Justinian himself, contracted plague, but he was a robust fellow, it seems. He fully recovered. Perhaps Europe’s first experience with small pox in the 2nd century was also roughly like that. The virus likely came up from Africa and swept through an immunologically naïve population. Japan’s first experience with small pox in the 8th century, meanwhile, might have been concentrated on young males, but there is evidence that it otherwise affected rich and poor alike. Overall, about one third of the population perished. The toll ultimately included all four brothers of the most elite of the elite noble families, the Fujiwara.
Meanwhile, the death tolls of other pandemics have concentrated themselves in certain segments of populations. The toll of the Spanish Flu (2018-2020), for example, was concentrated on people in their physical primes. The CDC guesses that the median age of death among Americans was 28. Very young people and elderly people were largely spared. The question of why remains a deep puzzle.
It is a blessing that the coronavirus toll has been concentrated on the most elderly cohorts in each country’s population. That may sound harsh, but the alternatives are harsher. The alternatives would be to concentrate the toll on younger people—people who would yet have the most years of high-quality life ahead of them.
In this essay I update results that I have reported this last January and in January 2021. I also include some new results about the age distribution of fatalities attributed to COVID. These results also reveal that, even absent COVID, younger people have been persistently dying at elevated rates from the beginning of the coronavirus pandemic right up to the present. This is a very bad result, because it indicates that something sinister other than COVID itself is harming the population. A likely suspect would be the public policy response to the pandemic. The precise “how” and “why” of that is something the health authorities, including the CDC and Anthony Fauci’s fiefdom, the NIH, should be made to speak to. They are not things that the publicly available data from the CDC enable us to tease out. Even so, the publicly available data reveal vivid signals that more than one bad thing is happening. Can the authorities be compelled to acknowledge this?
I also present new results about mortality derived from “Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified”. Fatalities from such mysterious conditions have exhibited regular, seasonal variation. Baseline rates have ranged between 560 per week in June and 680 per week at the very end of December. Starting in May 2021, however, weekly rates started to increase exponentially, exceeding 3,000 per week by the end of the year. The rate continued to increase into 2022.
Finally, I present new results about fatalities from “unnatural causes.” Unnatural causes would include deaths by suicide, alcohol poisoning, and drugs. Fatalities by unnatural causes started to surge right after the advent of COVID in 2020, and they appear to have been concentrated among younger people.
I identify five propositions and then present evidence for each proposition further below:
Proposition 1: The death toll from the “jab” exceeds 43,000 as of February 26, 2022.
At the beginning of May 2021, the vaccinated have started dying at accelerating rates discernible in CDC data on mortality. By January 1, 2022, they started dying at a rate well in excess of nearly 2,400 per week.
Proposition 2: Public policy interventions have had no discernible effect on the diffusion of coronavirus or on its effects on the population.
I show that performance across states has appreciably converged on the country-wide average. I use “excess mortality” by state as a measure of performance. There may have been variation in the approaches of states to COVID, but, over time performance state by state tends to converge on similar results. So, did public interventions make any difference or even make things worse? As I explained in an earlier essay[1]:
One state might feature a population that is more susceptible to COVID infection than that of another state. States like Florida and Arizona, for example, feature disproportionately high numbers of older retirees. At the same time, however, the climates and living styles of people in such places may afford them some protection from viral infection. In any case, the population of any given state and a state’s attributes may influence the trajectory of COVID in that state. Certain states will naturally feature higher rates of morbidity in a given year, and others, on average, will tend to feature lower morbidity. But, as coronavirus had become more widely dispersed across the country, did some states tend to perform proportionally better than others? Florida, for example, may experience higher-than-average morbidity in any given year, and one can only guess (correctly, it turns out) that rates of morbidity increased in 2020 and 2021. But, did those rates increase (again, proportionally) more than, say, in California?
Examining excess mortality in proportion to baseline mortality amounts to a kind of fixed-effects analysis in that it goes some way toward controlling for differences across states. For each state I calculate total, all-cause excess mortality in 2020-2021 and pose benchmark mortality for 2020-2021. I then take the ratio of excess mortality to benchmark mortality. I pose that ratio as a running measure of performance.
…
I establish the pre-COVID benchmark by examining total mortality by state for the years 2015-2019. In 2015 total mortality country-wide discernibly edged up from pre-2015 to a new plateau of about 2.8 million fatalities a year. The oldest baby boomers may have started retiring in large numbers, and that may have induced a “new normal” of higher mortality. From 2015-2019, however, total mortality has edged up merely as population has edged up. It is only after April 2020 that total mortality country-wide starts to exhibit some obvious irregularity.
The data from some number of the states are censored, but data from most of the larger states permit useful comparisons. We find that New York had the appearance of performing very badly in the early stages of the pandemic, which should not be surprising, because New York was the largest state that had been most heavily affected by COVID in the early going. But, over nearly two years the performance in New York converged on that of the entire country. Meanwhile, observers in the establishment media complained about performance in Florida while praising performance in New York and California. But, after two years the performance in all three states has converged on the national average. One could even argue that Florida continues to marginally outperform California and even that New York has marginally outperformed both Florida and California notwithstanding the fact that it started out so badly. That all goes toward saying that public policy responses have not made a discernible difference.
Proposition 3: The coronavirus phenomenon has induced fatalities that would not have otherwise occurred in 2020 or 2021.
Indeed, the coronavirus phenomenon was more than a non-event. It did not merely involve relabeling fatalities that would have otherwise occurred. It did involve an appreciable volume of fatalities that would not otherwise have occurred, although the phenomenon is complex. It involves well more than just bean-counting.
I examine total mortality in the United States from all causes in years 2015 through 2021. I then calculate benchmark mortality for the years preceding the COVID pandemic (2015 through 2019), and I then project that benchmark on to the years 2020 and 2021. The difference between projected, benchmark mortality and actual mortality constitutes “excess mortality”. Excess mortality is the volume of deaths that exceed expectations; the benchmark indicates expected mortality.
Proposition 4: Many, and possibly most, fatalities attributed to COVID would nonetheless have resulted from other causes had there been no pandemic.
The coronavirus phenomenon may have induced an appreciable volume of excess mortality, but we cannot count all coronavirus fatalities—possibly not eve most coronavirus fatalities—in excess mortality. There is a lot more going on in the data than simple bean-counting would reveal.
Proposition 5: Public policy interventions, and not COVID itself, have induced an appreciable number of fatalities among younger people.
We may not be able to definitely sort out the contribution of COVID to excess mortality, but the data do allow us to definitely observe that causes other than COVID have induced younger people to die at persistently elevated rates from the beginning of the pandemic and through 2020 and 2021. Absent access to more granular data—data that the government authorities sit on—we cannot definitively identify the exact sources of this persistent excess mortality among younger people, there is evidence, however, consistent with the proposition that suicides have appreciably increased starting in April 2020. Be that as it may, one can very well guess that public interventions (lockdowns and such) as well as adverse reactions to the vaccines have something to do with excess mortality among younger people.
Data and Evidence —
On to the evidence.
Proposition 1: The death toll from the “jab” exceeds 43,000 as of February 26, 2022.
I merge data from two CDC tables, “Weekly Counts of Deaths by State and Select Causes, 2014-2019” and “Weekly Provisional Counts of Deaths by State and Select Causes, 2020-2022”. One can access these data at https://data.cdc.gov/NCHS/Weekly-Counts-of-Deaths-by-State-and-Select-Causes/3yf8-kanr and https://data.cdc.gov/NCHS/Weekly-Provisional-Counts-of-Deaths-by-State-and-S/muzy-jte6. The CDC updated these tables as of March 16, 2022.
These data feature weekly counts of fatalities by state assigned to fifteen categories. Those categories are:
All Cause
Natural Cause
Septicemia (A40-A41)
Malignant neoplasms (C00-C97)
Diabetes mellitus (E10-E14)
Alzheimer disease (G30)
Influenza and pneumonia (J09-J18)
Chronic lower respiratory diseases (J40-J47)
Other diseases of respiratory system (J00-J06, J30-J39, J67, J70-J98)
Nephritis, nephrotic syndrome and nephrosis (N00-N07, N17-N19, N25-N27)
Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00-R99)
Diseases of heart (I00-I09, I11, I13, I20-I51)
Cerebrovascular diseases (I60-I69)
COVID-19 (U071, Multiple Cause of Death)
COVID-19 (U071, Underlying Cause of Death)
Taking the difference between “All Cause” and “Natural Cause” allows one to generate a 16th category, “Unnatural Cause.” Unnatural causes would include suicide, drug overdoses and alcohol poisoning.
For each of the sixteen categories, I calculate benchmark mortality using data from the six years preceding the pandemic, 2014-2019. I then project that benchmark into 2020 and 2021. The benchmark in 2020 and 2021 amounts to a prediction of the volume of deaths that would have occurred absent the pandemic. I then examine the difference between benchmark mortality and actual mortality in 2020 and 2021. This difference is a measure of “excess mortality,” the volume of fatalities in excess of what one would have expected.
Mortality in the United States exhibits obvious seasonality, with weekly mortality using peaking in January/February and reaching annual lows in July/August. To accommodate this seasonality, I fit a regression equation that features a sine wave. The regression also includes a time trend to accommodate population growth from year to year. Fitting the regression equation amounts to calculating benchmark mortality.
The CDC itself recognizes that there is no unique way to calculate benchmark mortality. A common alternative would be to compare mortality in 2020 and 2021 to average mortality in the preceding few years. I have sometimes done this kind of exercise myself, and it yields results consistent with those derived by applying regression equations.
To give the reader the basic idea about what calculating excess mortality involves, consider the following graph.
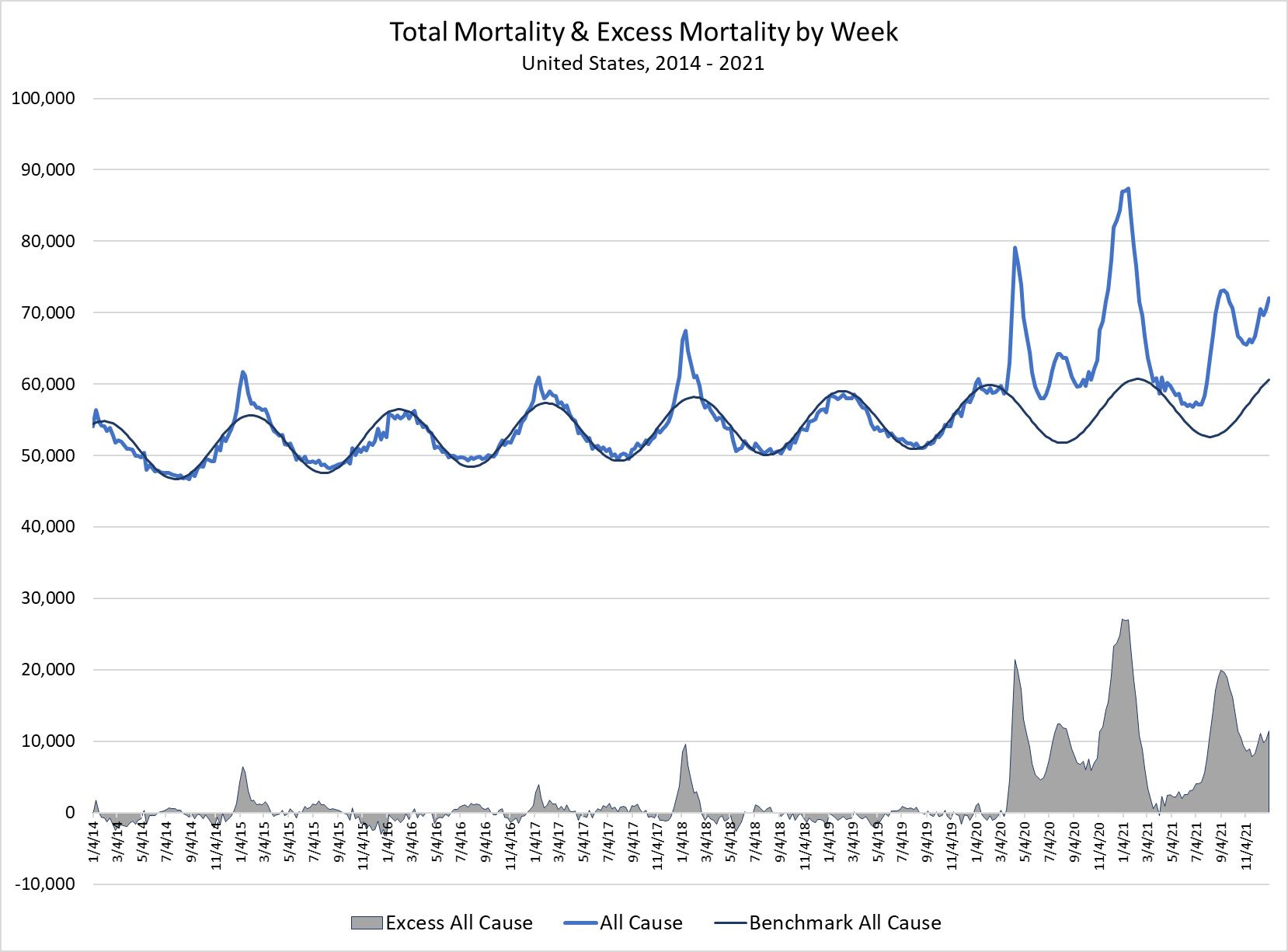
The blue line indicates weekly mortality from all causes. A striking feature of mortality is that it exhibits such strong seasonality. It peaks in January of each year and reaches a low in July/August. Mortality, it seems, follows the sun with a lag… and exposure to the sun also follows a sine wave. Hence the inclusion of a sine wave in a non-linear regression. That smooth curvy line indicates the fit of a regression equation featuring both a sine wave and a linear time trend to the mortality date pre-2020. It does not capture sharp deviations from benchmark mortality. How could it? Some seasons are just bad, like the cold-and-flu seasons of early 2015 and early 2018. Some cold-and-flu-seasons are mild, such as those of 2016, 2019 and early 2020.
I project the fitted curve into 2020 and 2021. The gray area indicates those deviations of actual, all-cause mortality from benchmark mortality. Excess mortality deviates sharply from benchmark mortality in March 2020, just as COVID fatalities start to ramp up.
One can see that excess mortality remained sharply positive over the next year, only touching the benchmark in March of 2021. It then ramps up again before moderating, but it remained sharply positive for the remainder of 2021.
We will return to a graph much like this one later, but for now let me indicate that I have endeavored to characterize baseline rates of mortality by specific disease categories, not just of “all cause” mortality.
The following graph maps out weekly fatalities attributed to “diseases of the heart.”
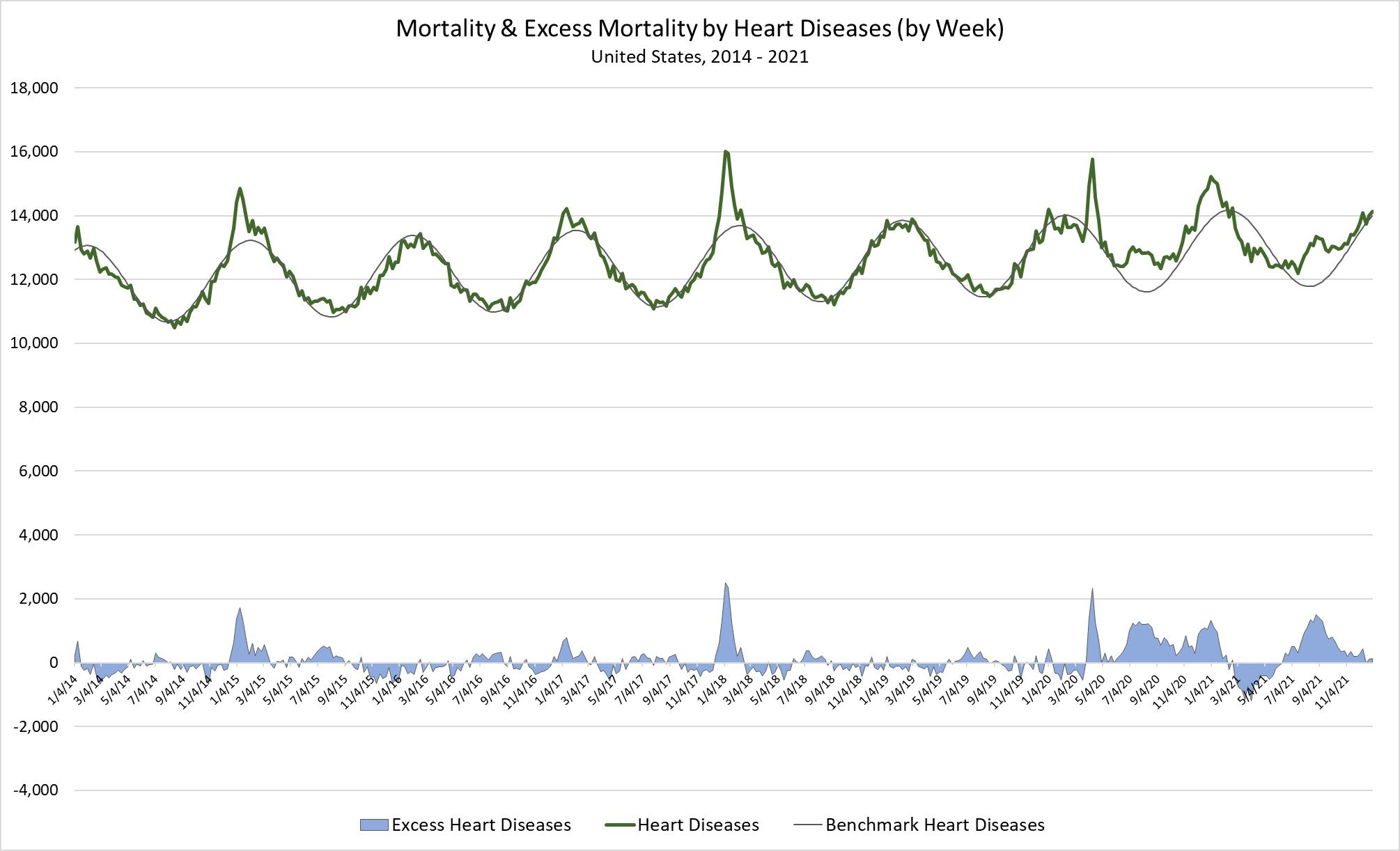
“Diseases of the heart” account for more than 20% of all-cause mortality, and, like all-cause mortality, it exhibits obvious seasonality. As above, the smooth, curvy line indicates a measure of benchmark mortality, and the blue area indicates excess mortality.
One can observe a spike in fatalities attributed to heart diseases in April 2020, and thereafter fatalities by heart diseases generally exceed the benchmark—except in the spring and early summer of 2021. The count of fatalities attributed to heart diseases runs far below the benchmark before surging again and peaking in late August 2021.
The coronavirus phenomenon obviously influences the incidence or attribution (which may be questionable) of fatalities to heart diseases, but the point here is to show that the regression method captures the unusual trajectory of excess mortality of heart diseases after the advent of COVID. Of real interest, however, are applications of the same method to the category “Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00-R99).” Consider the following graph:
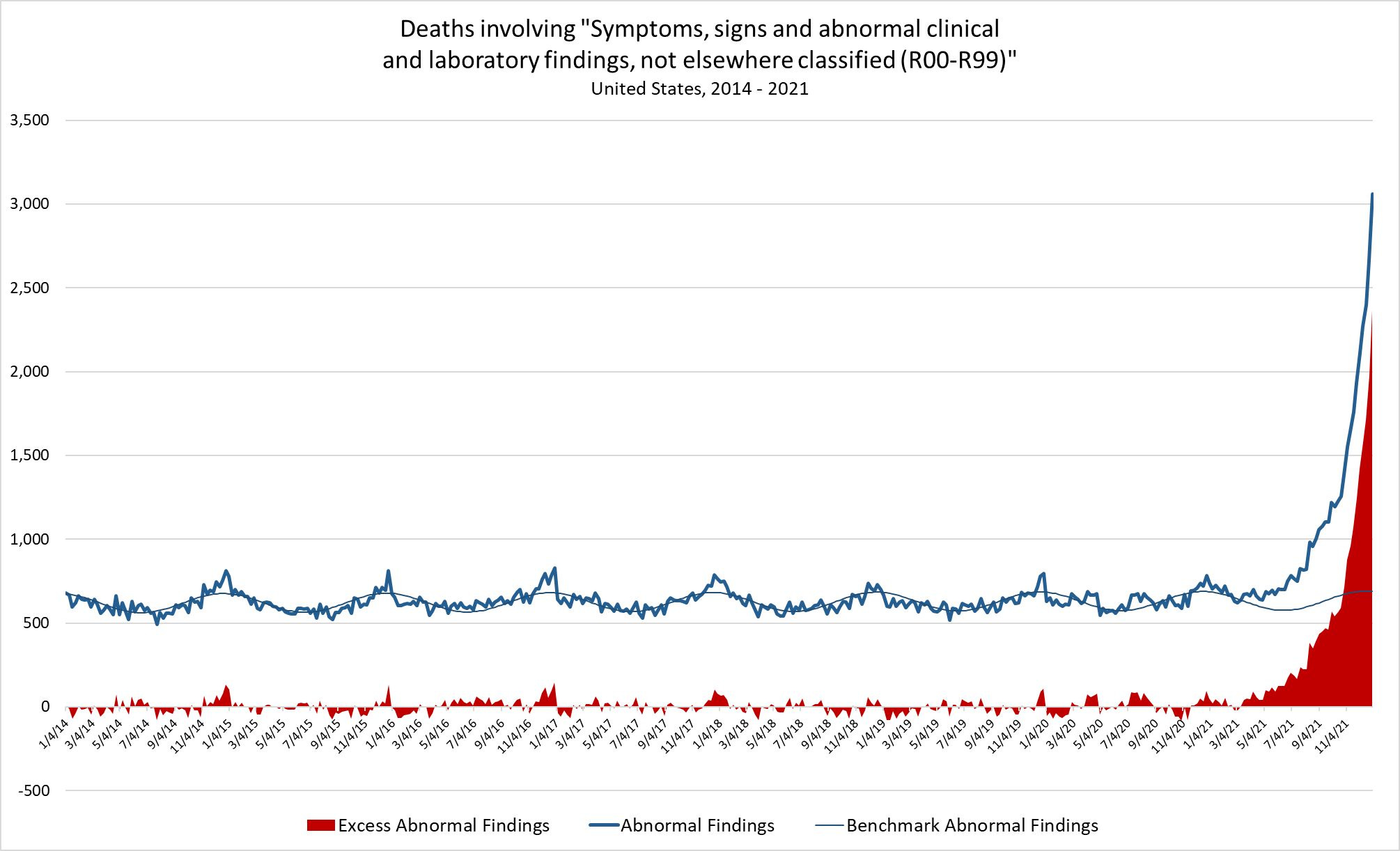
Fatalities involving “Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified” constitute about 1% of all fatalities. They also exhibit obvious seasonality. The most striking feature of these data, however, is that they deviate sharply from the benchmark starting in March 2021—one year after the advent of the COVID pandemic in the United States. Not only did fatalities attributed to other “abnormal… findings, not elsewhere classified” start to deviate in March 2021, but they started to ramp almost exponentially. Weekly, baseline rates of would vary, year to year, between 580 and 690, but, by the end of 2021 the weekly rate exceeded 3,000 and showed no evidence of leveling off. Excess mortality by “abnormal” causes closed out the year in excess of 2,300 per week. More than 21,000 excess “abnormal” fatalities racked up from the middle of March to the end of the year.
What to make of this? What could have been happening? Why do we not see such a spectacular deviation in the CDC data over the course of the previous seven years?
It is hard not to think that we are witnessing the effects of the COVID vaccines (the mRNA gene therapies). Meanwhile, add to the toll of 21,000-plus in 2021 the under-tabulated toll of another 23,000 in excess fatalities in 2022 as of February 26, 2022. That would bring the toll of the vaccines attributed to “abnormal” causes to more 43,000 as of late February 2022.
Let’s now turn to the second proposition.
Proposition 2: Public policy interventions have had no discernible effect on the diffusion of coronavirus or on its effects on the population.
To explore this proposition, I use CDC data titled “Weekly Counts of Deaths by Jurisdiction and Age,” available at https://data.cdc.gov/NCHS/Weekly-Counts-of-Deaths-by-Jurisdiction-and-Age/y5bj-9g5w (updated as of March 16, 2022).
These data include counts of all-cause mortality by week and by state from the first full week of 2015 through 2021. I apply the non-linear regression model to each of the fifty states as well as Puerto Rico and the District of Columbia. Data reported for some of the states were censored or otherwise problematic. I thus exclude five states from the analysis: New Hampshire, North Dakota, Vermont, Tennessee, and Wyoming.
In this first graph I feature excess mortality for large states as it accumulated over time. The point here is more expositional, to show that looking at accumulated excess deaths by state really doesn’t reveal any way to compare performance across states. Other things equal, bigger states may very well experience larger numbers of fatalities (and excess fatalities) over time. Some states may feature more vulnerable populations and would thus appear to perform poorly relative to other states. Thus, consider this graph:
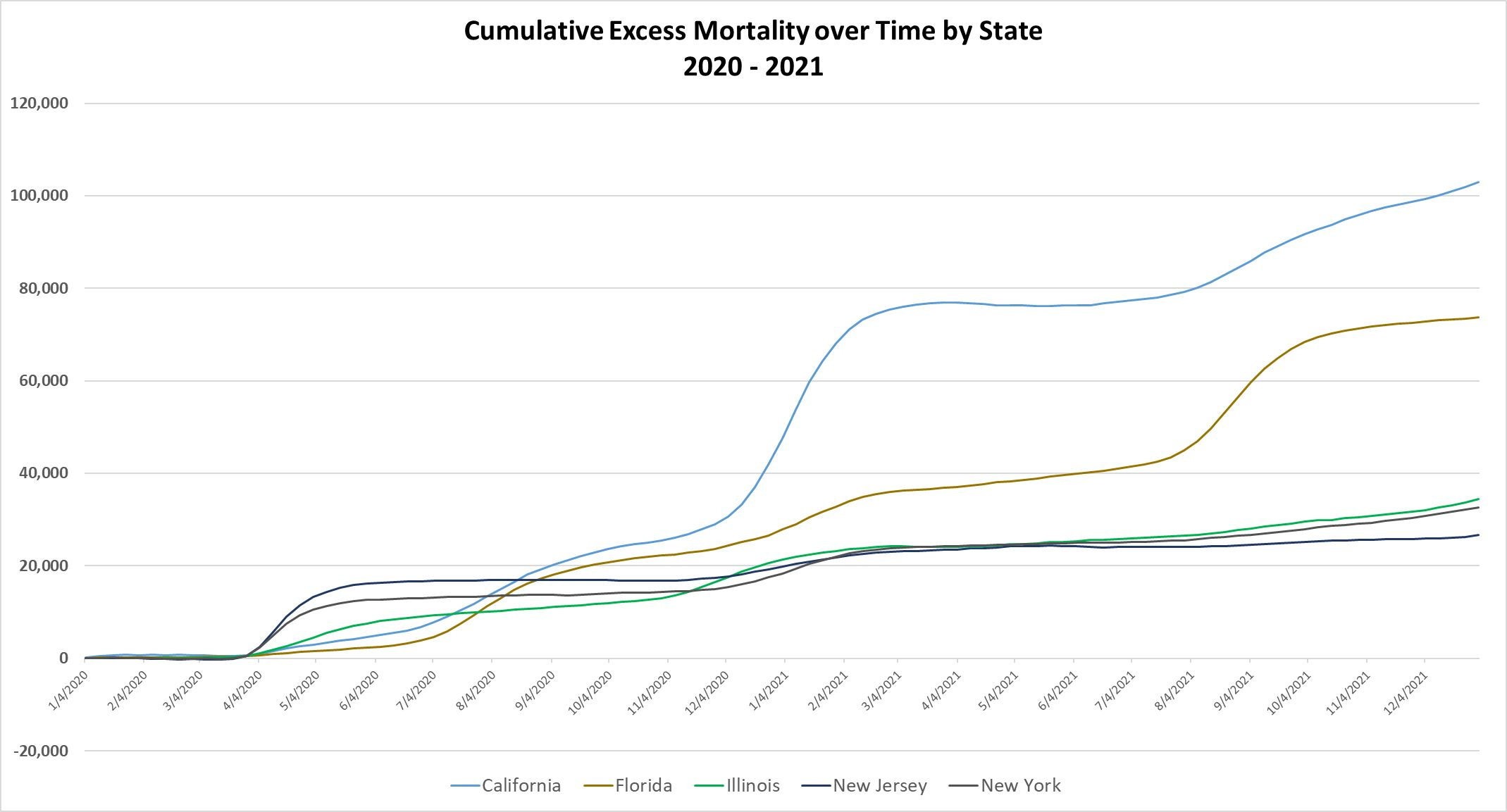
One might be tempted to suggest that California has performed worse than Florida (and Illinois, New Jersey and New York) to date, because it has experienced more excess mortality by the end of 2021. Indeed, California would appear to have started performing more poorly than these other states in August 2020. But, if we take the ratio of a state’s accumulated excess mortality to its accumulated benchmark mortality, then we might effectively control for certain differences between states that are fixed over the two years 2020 and 2021. The next graph features just such proportionally-adjusted excess mortality over time for these five states. This graph also includes the United States. The United States taken as a whole effectively amounts to taking a weighted average of all states and territories.
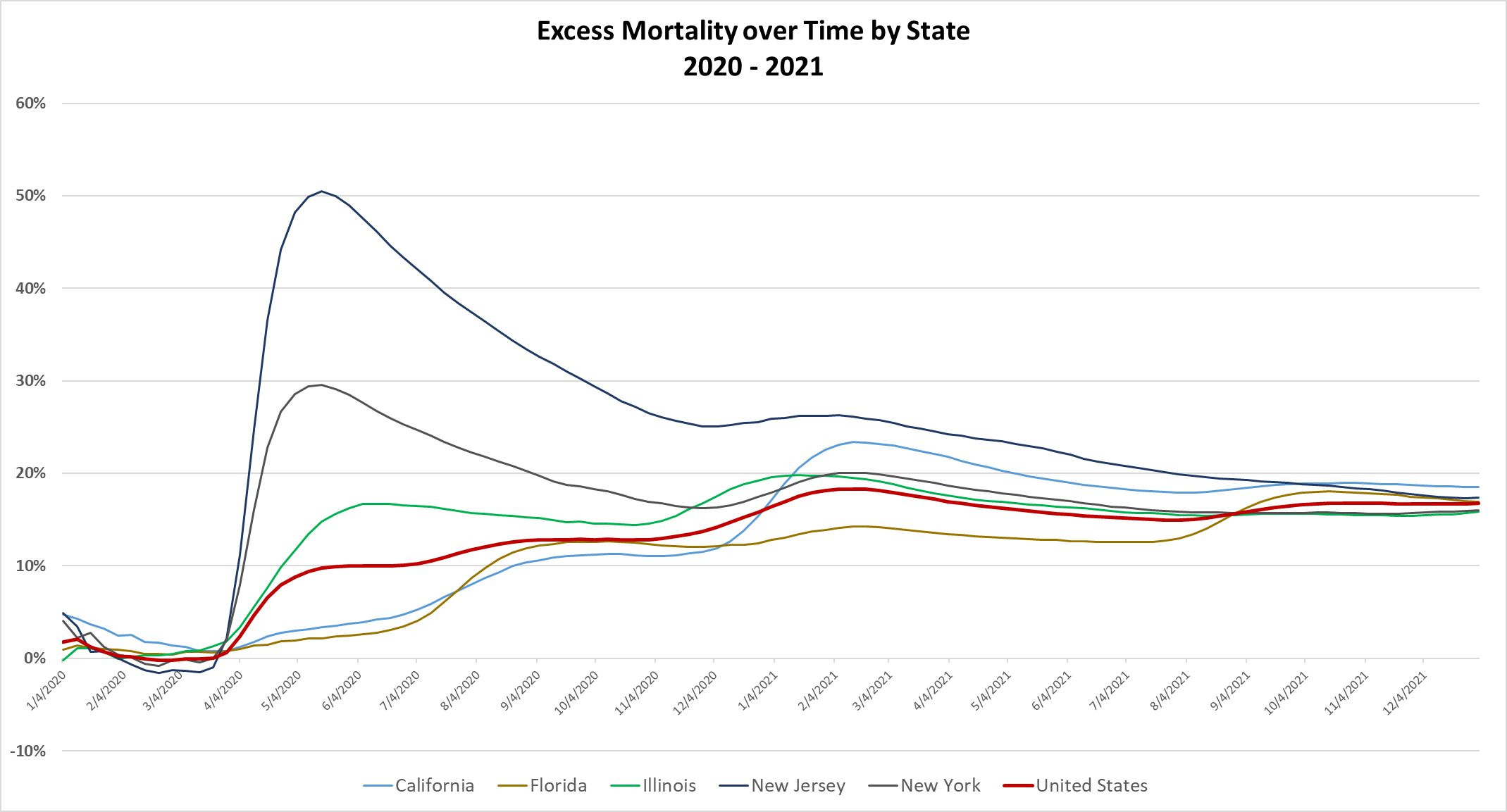
In this graph New Jersey appears to be performing very badly relative to the other states in the few months after the advent of COVID in the United States. By the middle of May 2021, New Jersey experienced total mortality that was more than 50% greater than its projected, benchmark death toll through the first four-and-a-half months of 2021. By the end of 2021, however, New Jersey fared much better. Over the course of the entire year, it experienced about 26% total mortality in excess of its projected total mortality for the year. By the end of 2022, New Jersey experienced total mortality 17.4% in excess of the total mortality projected for the two years 2020 and 2021.
By the end of 2021, New Jersey ends up outperforming California in that California registered total mortality that was 18.5% greater than its projected, benchmark mortality for 2020-2021. California performed worse than the United States average in that the United States as a whole clocked in at 16.7% by the end of 2021.
Florida, meanwhile, ultimately clocked in at 16.9%, very close to the national average. New York performed slightly better than the national average, clocking in at 16.0%. Ultimately, these states appear to have performed about as well as each other after the virus had a chance to distribute itself widely in the populations of all states. States that were hit early have the appearance of performing very badly early on. But once the virus became more widely distributed, other states were not spared. The performance of all states thus appears to converge over time on the national average.
And what to make of that? Public, ostentatious displays of doing something; destructive policies like lockdowns and mandates… None of these had any effect on performance. The conceit that public officials could control the virus and achieve “Zero COVID” proved to be just that: a silly conceit. Zero COVID itself has proven to be a fool’s errand. It was predictable. It was predicted.
It is true that if one examines this measure of performance—excess mortality in proportional (%) terms rather than in absolute counts of fatalities—then a few states do stand out as better performances and others as worse performers. Hawaii, for example, clocks in at 4.82% by the end of 2021. That is exceptional, and it may be that Hawaii is exceptional. Because it is a relatively isolated cluster of islands? Because the sizable population of Pacific Islanders and East Asians (especially people of Japanese extraction) have proven to be more resilient in the face of COVID? Because people spend more time outside getting fresh air and exercise? Something else? At the other extreme is Alaska, clocking in at more than 25% at the end of 2021. Does it have something to do with climate? Unlike those Hawaiians, do the Alaskans spend more time in doors during certain times of the year? So, not all states have converged to points close to the United States average, but all states have demonstrated some convergence over time.
Proposition 3: The coronavirus phenomenon has induced fatalities that would not have otherwise occurred in 2020 or 2021.
Let’s return to analysis of excess mortality in the United States as a whole. The following graph features weekly mortality, benchmark mortality and excess mortality in the years 2015 through 2022. It also features two other items: total mortality less fatalities attributed principally to COVID (“by COVID”) and total mortality less fatalities either “by COVID” or “with COVID”.
Again, I use CDC data titled “Weekly Counts of Deaths by Jurisdiction and Age,” available at https://data.cdc.gov/NCHS/Weekly-Counts-of-Deaths-by-Jurisdiction-and-Age/y5bj-9g5w (updated as of March 16, 2022).
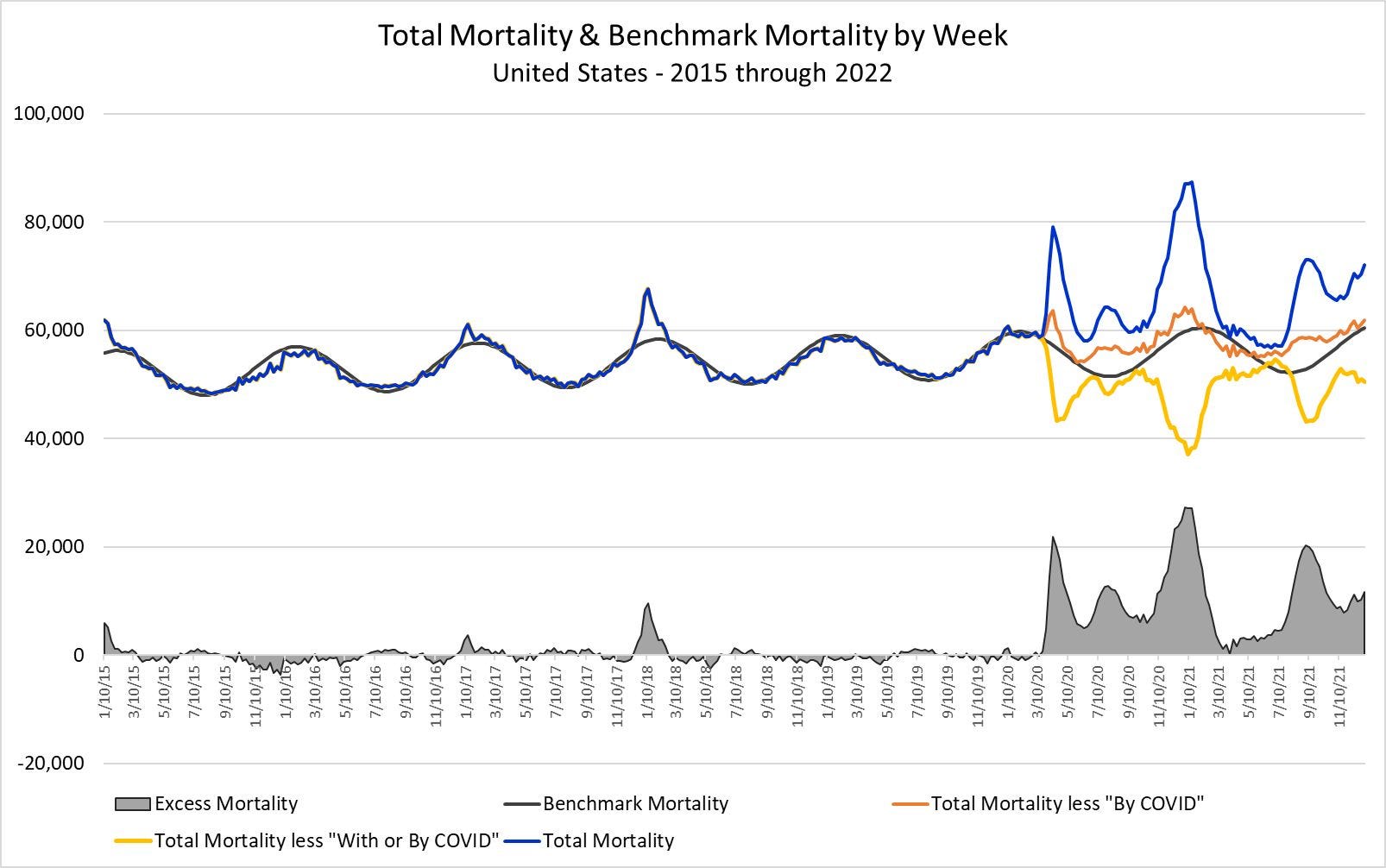
Note that the yellow line, “Total Mortality less ‘With or By COVID’,” almost uniformly runs below benchmark mortality. The area between that yellow line and benchmark mortality indicates the volume of people who likely would have died by some cause other than COVID had COVID never arrived. In 2020 that number of fatalities would have been nearly 270,000. In 2021 that number would have been well more than 360,000. Thus, in 2020 and 2021, about 630,000 people who died “With or By COVID” would likely have died anyway.
Within that 630,000, we can’t distinguish between people who died “With COVID” from those who died “By COVID”. We also know that nearly 850,000 people died “By COVID” in 2020/2021, but it would wrong to say that almost all of those people would likely be living now absent the advent of COVID. Again, likely hundreds of thousands of them belong to the 630,00 who would have died anyway. Thus, to argue that the toll of COVID in 2020/2021 was 850,000 merely amounts to manipulation. Many of those 850,000 really were people who very seriously immunocompromised and not likely to live out the year.
This last observation sets up the fourth proposition.
Proposition 4: Many, and possibly most, fatalities attributed to COVID would nonetheless have resulted from other causes had there been no pandemic.
We cannot deny that the coronavirus phenomenon did induce a sizable volume of excess mortality, but what might one mean by “coronavirus phenomenon?” In 2020/2021, excess mortality was about 985,000. That toll is greater than the toll of mortality “By COVID” itself. Much of that toll of 985,000 surely derived directly from COVID itself. But, note how complex the coronavirus phenomenon is. A large volume of people in that toll of 985,000 died from causes other than COVID. At least 135,000 had died from something elsewhere, and, a few hundred thousand more of those 985,000 also died from something else. It is even conceivable that most of those people in the 985,000 died from something other than COVID. We just can’t determine how many. But, even so, what did they die from? And why did they die? Did poor public policy have something to do with it?
Proposition 5: Public policy interventions, and not COVID itself, have induced an appreciable number of fatalities among younger people.
The COVID experiences for older age cohorts look qualitatively the same in the CDC data for people over age of 44. The magnitudes may vary, but the picture tells very much the same story cohort to cohort.
Consider the following graph for people aged 65-74:
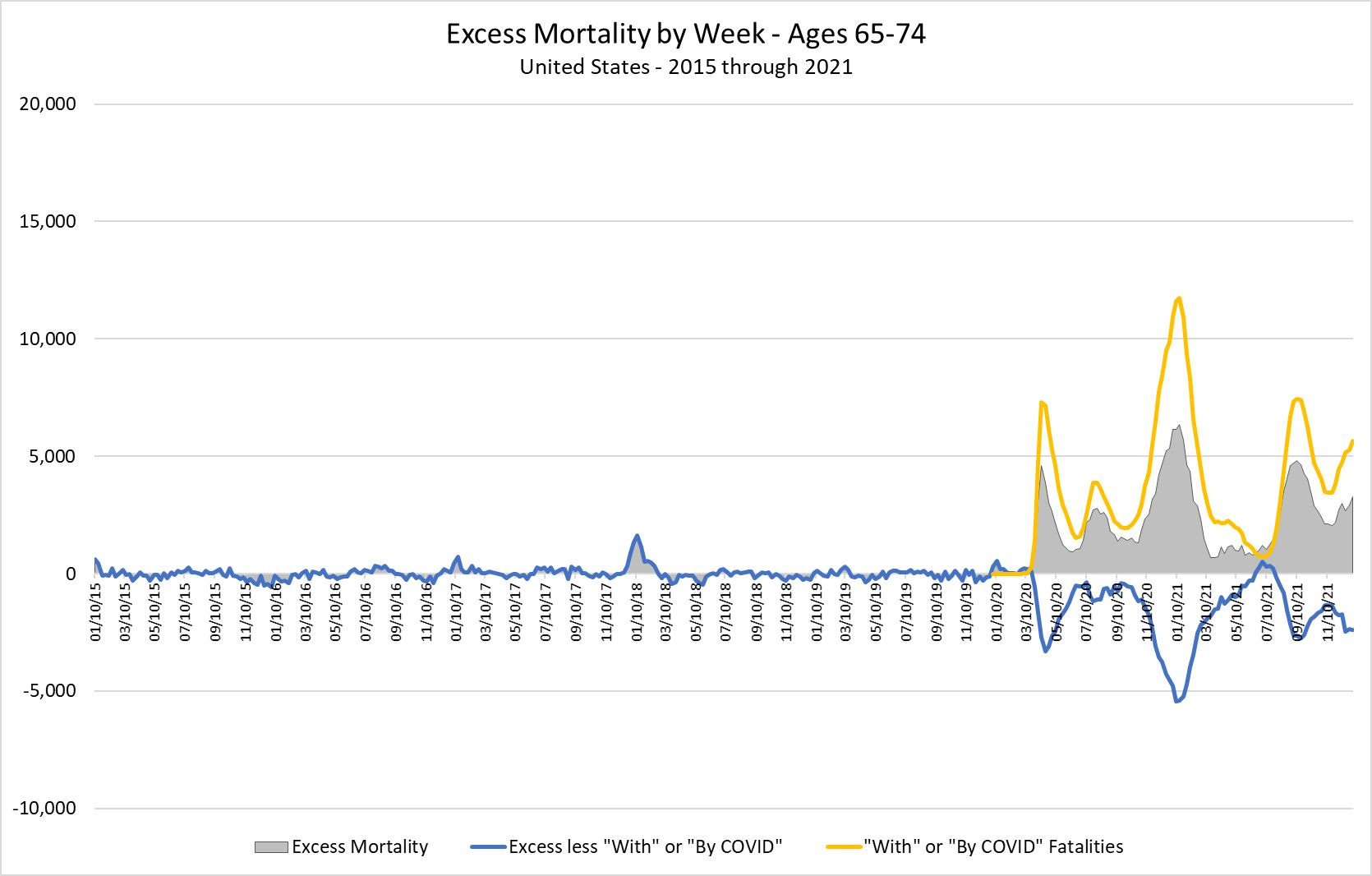
The grey area indicates excess mortality by week. The yellow line indicates mortality “With COVID” or “By COVID”. The blue line indicates Excess mortality less that mortality “With COVID” or “By COVID”. The fact that (1) the yellow line generally exceeds excess mortality and (2) blue line generally runs negative after the advent of COVID indicates that a lot of people who died either “With COVID” or “By COVID” would have died anyway—but not all of them; excess mortality was not positive for no reason.
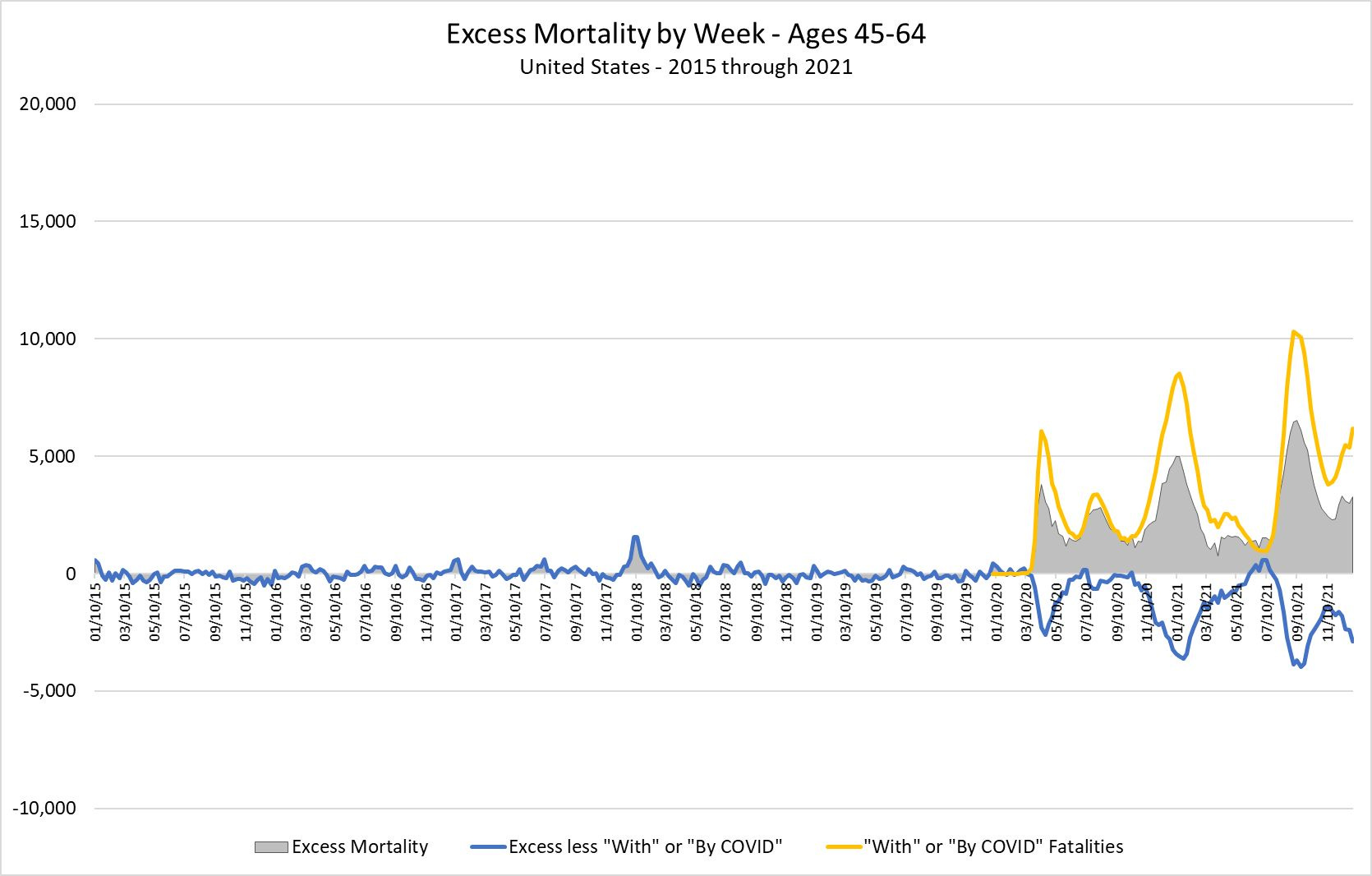
The graphs for people age 45-64, 75-84 and 85-plus look much the same. Here, for example, is the graph for people aged 45-64. A difference is that excess mortality for this cohort increased in late 2021.
The picture literally starts to look much different when we examine younger people. The CDC data permit some visibility into two younger age cohorts, people aged 25-44 and people aged 0-24. First consider excess mortality for people of prime working age, people aged 25-44:
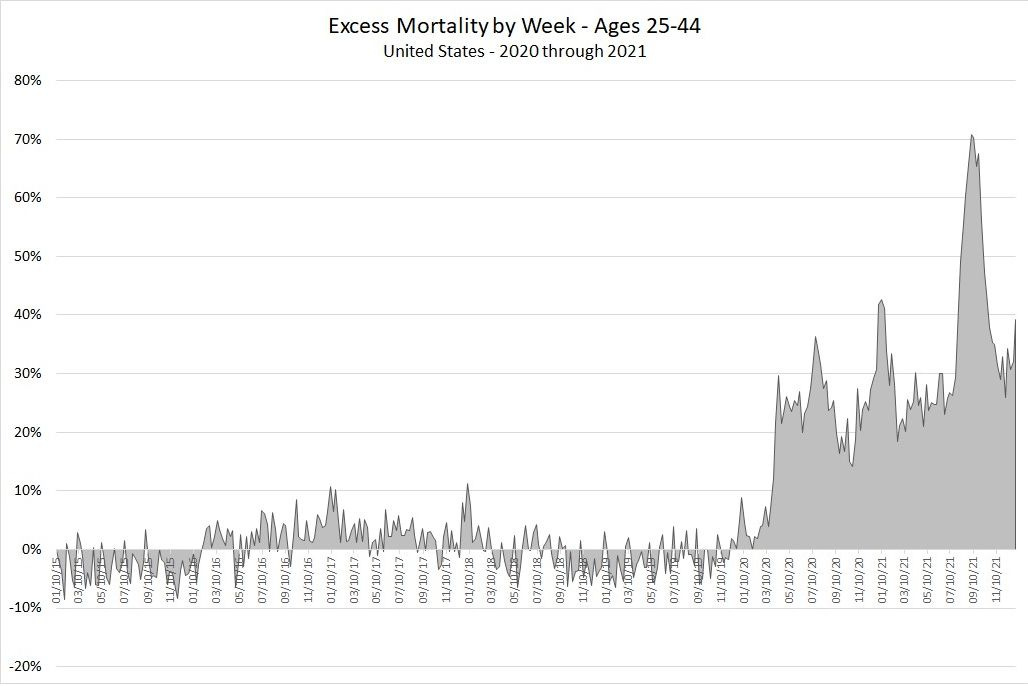
Excess mortality exhibits some of the peaks associated with COVID fatalities, but the excess mortality appears to reached a persistently high plateau of 20% above benchmark mortality. Something other than COVID seems to be going on.
Let’s look at these same data again, but, this time, let’s add COVID mortality and excess mortality less COVID:
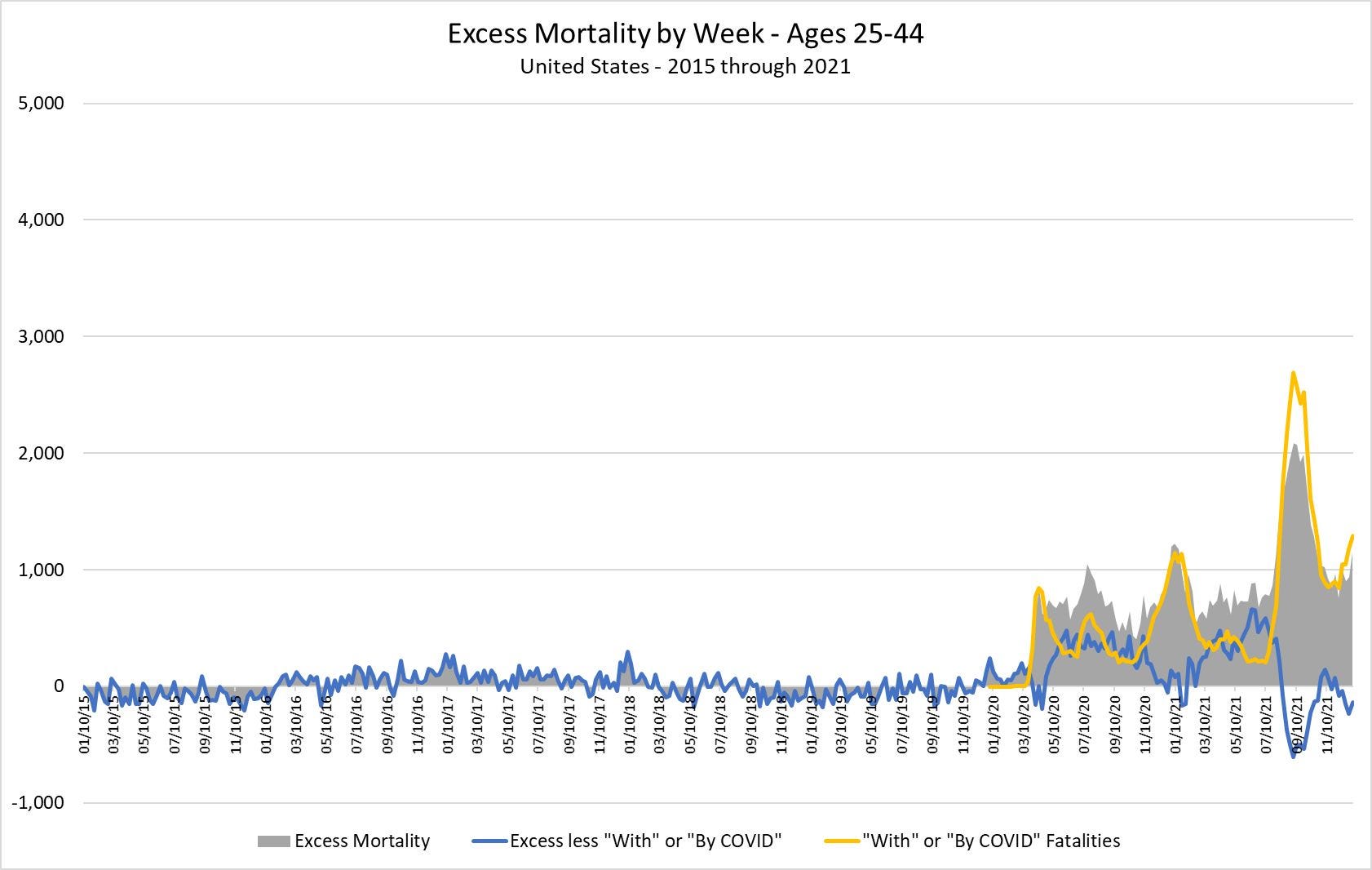
The blue line is no longer generally negative after the advent of COVID. If anything, it spends more time being positive than negative. That means people had been dying in elevated numbers from something other than COVID. Hold that thought. Note also that the data indicate that these people suffered their worst experience with COVID around September 2021. Were these people really suffering from COVID, or were they suffering vaccine-induced effects just as everyone got vaccinated in time for the new school year?
Now, let’s look at the age cohort 0-24:
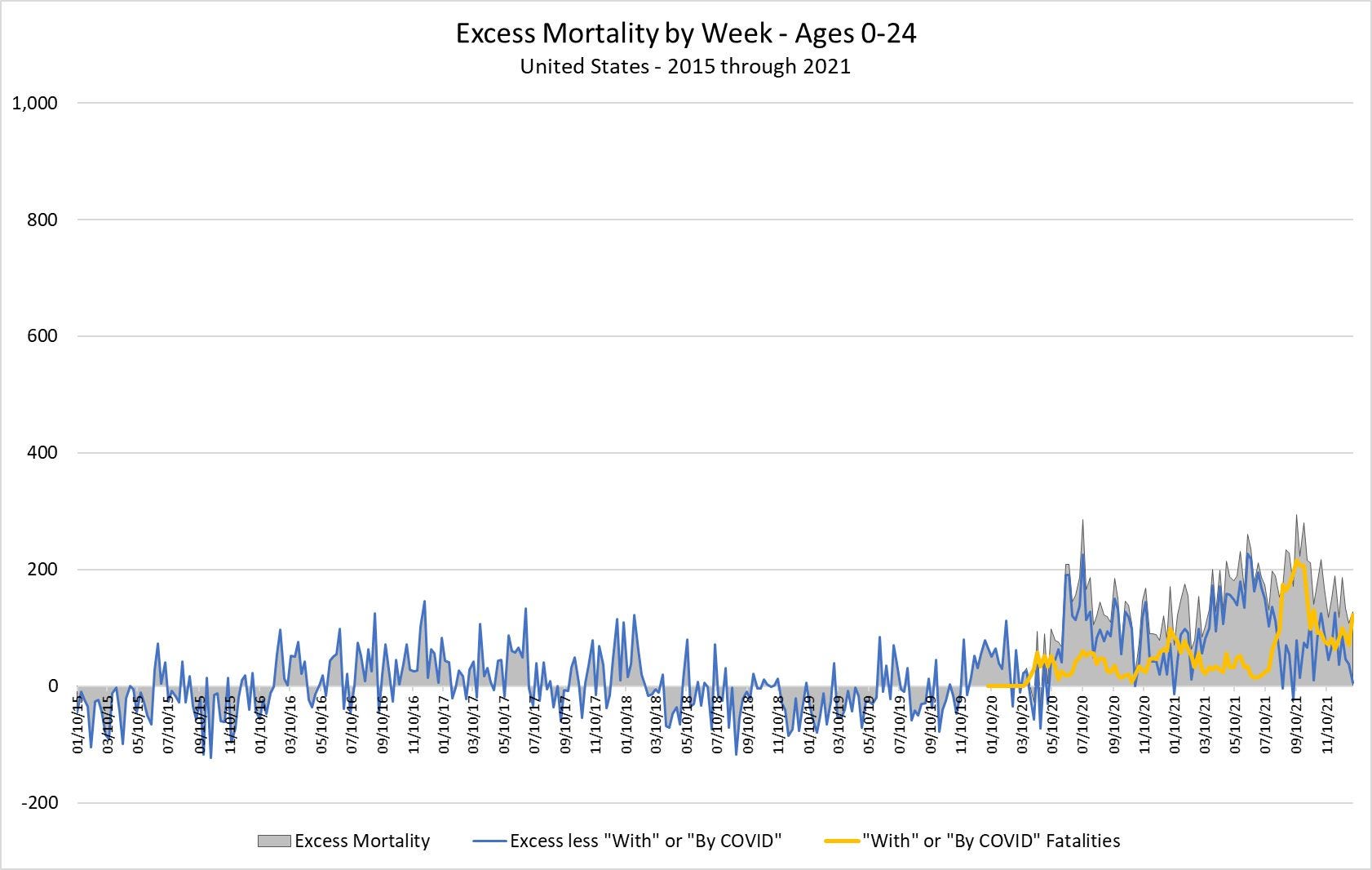
The numbers are more modest for the youngest people—no surprise—but note that the CDC does not attribute most excess mortality to fatalities either “With COVID” or “By COVID” after the advent of COVID. Indeed, after the advent of COVID, very young people are dying at elevated rates—at rates exceeding another 100 people per week—by causes not relating to COVID. What is going on?
The following graph provides a clue.
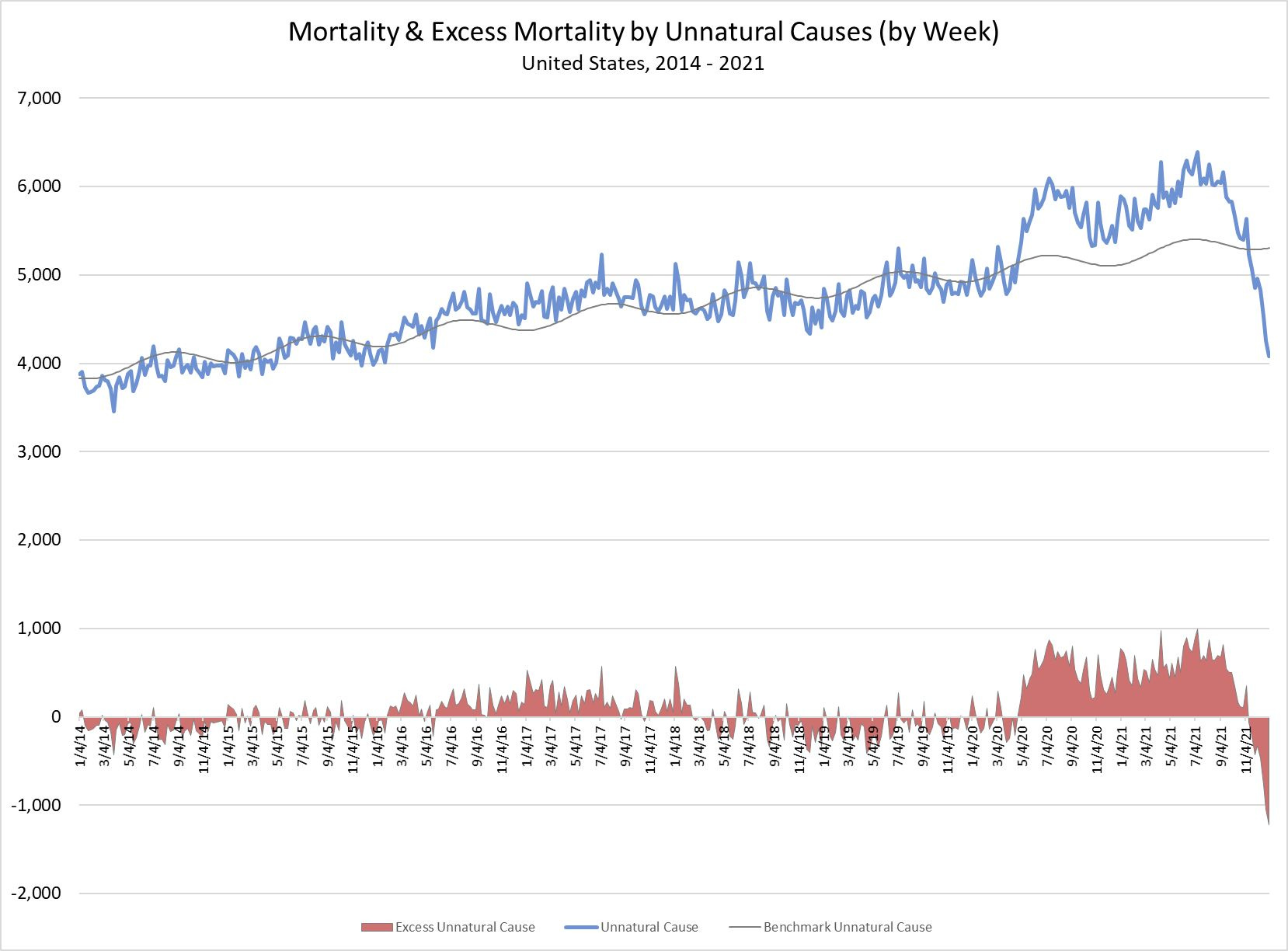
The red area indicates excess mortality by “Unnatural Causes”. Unnatural causes would include suicide, car accidents, and murder. The regression line does not fit these data as well as it fits other mortality data, but it renders a serviceable measure of excess mortality by unnatural causes, and it shows that deaths by unnatural causes appeared to increase by more than 500 per week above baseline rates from April 2020 through September 2020. It is only after September 2020 that deaths by unnatural causes fall off sharply; excess mortality turns sharply negative as the year 2021 closes out.
What is going on? It is hard not to suggest that closing schools and universities imposed a lot of stress on younger people; rates of suicide among younger people increased. Perhaps drugs and alcohol took their toll, too, but opening schools and universities in September 2021 relieved that stress. At the same time, however, younger people and working people started to experience the toll of the vaccines. The toll of the vaccines starts showing up in March 2021. That toll would have been concentrated on younger people; older people would more likely have opted in to the vaccine soon after the rollout of vaccines in late 2020. Deaths of despair and deaths induced by vaccines have disproportionately affected younger people and working people.
Conclusion —
In January I posted an essay titled “The COVID Children’s Crusade.” That essay took up clues in the Vaccine Adverse Effects Reporting System (VAERS) about the effects of the vaccines on younger people. The VAERS data are imperfect, but they serve an important purpose: They provide danger signals. The VAERS data have been screaming that something very bad is going on with the vaccines.
I opened that essay thusly:
In his semi-autobiographical account, Slaughterhouse Five, Kurt Vonnegut recounts being captured by the Germans during the Battle of the Bulge (1944) and then enjoying the privilege of joining POW's assigned to work in Slaughterhouse 5 in Dresden. The POW's ended up enjoying the greater privilege of being on the receiving end of the infamous firebombing of Dresden in 1945.
Kurt Vonnegut and his friend Bernard O'Hare made it out intact and eventually made it home by way of a Soviet prison camp.
Years later Vonnegut looked up his “old war buddy” O'Hare. He wanted to take some time with O'Hare to recount some of their experiences in the war. Those experiences would inform a book he had been struggling with.
“You were just babies in the war,” exclaimed O'Hare's wife Mary. This notion of “babies” going off to war got the three of them -- Kurt, Bernie and Mary -- thinking about the "The Children's Crusade":
O’Hare looked it up in a book he had, Extraordinary Popular Delusions and the Madness of Crowds by Charles MacKay [1841]… [T]he Children's Crusade started in 1213, when two monks got the idea of raising armies of children in Germany and France and selling them in North Africa as slaves. Thirty thousand children volunteered, thinking they were going to Palestine...
Through a misunderstanding, some children reported for duty in Genoa, where no slave ships were waiting. They were fed and sheltered and questioned kindly by good people there -- then given a little money and a lot of advice and sent back home.
“Hooray for the good people of Genoa,” said Mary O'Hare.
The complete title of Slaughterhouse Five is Slaughterhouse-Five, or the Children's Crusade: A Duty-dance with Death.
Are not the public health authorities world-wide and their enablers in the political class intent on engaging a new Children’s Crusade? Specifically, does it really make sense to push the “vax” – the mRNA therapies – on young people?
The madness of crowds, indeed. The great puzzle is: Why have the public authorities, themselves seemingly mad, enabled this collective madness?
I posed a few narratives in this essay. They include:
(1) Public interventions to control COVID have had no positive effect. If anything, they have induced harm. Just look at the experiences across states. They demonstrate convergence over time, suggesting that there was no way the authorities could somehow contain the virus.
I note that humanity has managed to eradicate only two viruses, smallpox and rinderpest. Rinderpest affects livestock. But note all of the flu viruses, other coronaviruses, Ebola virus and such that we have not eradicated. We have not even managed to eradicate measles notwithstanding the fact that measles has no known, non-human reservoir to hide in. I learned that bit merely by punching the terms “measles” and “reservoir” into a search engine. A handful of research papers popped up. The experience with COVID is consistent with those of other viruses; the conceit of Zero COVID was just a conceit. But, again, why would the public authorities maintain this conceit when they likely knew better?
(2) The COVID phenomenon is well more complicated than mindless bean-counting alone would suggest. There is more to the coronavirus phenomenon than just counts of fatalities attributed to COVID. There is a direct toll of COVID-induced fatalities, but then there is the question of whether public interventions either aggravated or mitigated the toll of COVID-induced fatalities. Further, there is the question of whether public interventions aggravated the toll of non-COVID fatalities. Did an appreciable volume of people of prime working age succumb to other conditions? Did alcohol, drugs and suicide take their tolls among people who had been cast of work or had lost their businesses? Did the campaign to get people “vaccinated” with the mRNA therapies take an appreciable toll?
(3) School age people and people of prime working age have been made to bear most of the costs of poor public policy. They lost jobs and livelihoods. They lost contact with school friends. They’ve lost a few years of learning. Deaths of despair show up among these people, and adverse effects induced by the vaccines have been taking their toll. The vaccine toll is still rising.
The publicly available data reveal obvious signals that something very bad is going on—obvious to anyone who takes the time to pay attention and look. Meanwhile, the public authorities, including the CDC and NIH, sit on top of much more granular data that would enable researchers to better discern the effects of public policy decisions. Absent being compelled, the authorities are never going to produce useful data or useful analysis. The New York Times pretended to be surprised that the authorities withhold data. In an essay titled, “The New York Times gets it … sort of,” I made the point that the authorities always withhold data. That conforms to standard operating procedure. Indeed, the CDC even offers an excuse. It complains that affording better access to data would merely allow people to “misinterpret” those same data; the authorities, the self-anointed experts, must maintain their monopoly over the data. They are afraid of being found out for the incompetent frauds they are.
[1] “The Orpheus Fallacy: Confusing Correlation with Causality in COVID Interventions,” January 13, 2022.
I believe the R00-R99 category is a holding category until diagnosis is confirmed. It always appears raised at the current date. Great work..
It Takes a Village of Bureaucrats to Implement Medical Despotism
AMA = American Mafia Association
CDC = Center for Death and Corruption
FDA = Fraud and Death Association
HHS = Holistic Humanicide Services
MD = Moral Deficiency
NIH = Nihilism In Healthcare